Manual of Surgery by Alexis Thomson (book recommendations for young adults .TXT) 📖

- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery by Alexis Thomson (book recommendations for young adults .TXT) 📖». Author Alexis Thomson
Structure of Skin.—The skin is composed of a superficial cellular layer—the epidermis, and the corium or true skin. The epidermis is differentiated from without inwards into the stratum corneum, the stratum lucidum, the stratum granulosum, and the rete Malpighii or germinal layer, from which all the others are developed. The corium or true skin consists of connective tissue, in which ramify the blood vessels, lymphatics, and nerves. That part of the corium immediately adjoining the epidermis is known as the papillary portion, and contains the terminal loops of the cutaneous blood vessels and the terminations of the cutaneous nerves. The deeper portion of the true skin is known as the reticular portion, and is largely composed of adipose tissue.
Blisters result from the exudation of serous fluid beneath the horny layer of the epidermis. The fluid may be clear, as in the blisters of a recent burn, or blood-stained, as in the blisters commonly accompanying fractures of the leg. It may become purulent as a result of infection, and this may be the starting-point of lymphangitis or cellulitis.
The skin should be disinfected and the blisters punctured. When infected, the separated horny layer must be cut away with scissors to allow of the necessary purification.
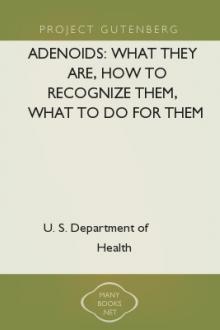
Fig. 93.—Callosities and Corns on the Sole and Plantar Aspect of the Toes in a woman who was also the subject of flat-foot.
Callosities are prominent, indurated masses of the horny layer of the epidermis, where it has been exposed to prolonged friction and pressure. They occur on the fingers and hand as a result of certain occupations and sports, but are most common under the balls of the toes or heel. A bursa may form beneath a callosity, and if it becomes inflamed may cause considerable suffering; if suppuration ensues, a sinus may form, resembling a perforating ulcer of the foot.
The treatment of callosities on the foot consists in removing pressure by wearing properly fitting boots, and in applying a ring pad around the callosity; another method is to fit a sock of spongiopilene with a hole cut out opposite the callosity. After soaking in hot water, the overgrown horny layer is pared away, and the part painted daily with a saturated solution of salicylic acid in flexile collodion.
Corns.—A corn is a localised overgrowth of the horny layer of the epidermis, which grows downwards, pressing upon and displacing the sensitive papillæ of the corium. Corns are due to the friction and pressure of ill-fitting boots, and are met with chiefly on the toes and sole of the foot. A corn is usually hard, dry, and white; but it may be sodden from moisture, as in “soft corns” between the toes. A bursa may form beneath a corn, and if inflamed constitutes one form of bunion. When suppuration takes place in relation to a corn, there is great pain and disability, and it may prove the starting-point of lymphangitis.
The treatment consists in the wearing of properly fitting boots and stockings, and, if the symptoms persist, the corn should be removed. This is done after the manner of chiropodists by digging out the corn with a suitably shaped knife. A more radical procedure is to excise, under local anæsthesia, the portion of skin containing the corn and the underlying bursa. The majority of so-called corn solvents consist of a solution of salicylic acid in collodion; if this is painted on daily, the epidermis dies and can then be pared away. The unskilful paring of corns may determine the occurrence of senile gangrene in those who are predisposed to it by disease of the arteries.
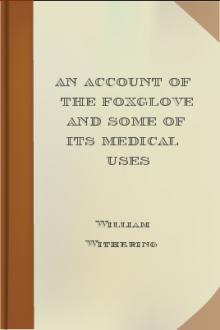
Chilblains.—Chilblain or erythema pernio is a vascular disturbance resulting from the alternate action of cold and heat on the distal parts of the body. Chilblains are met with chiefly on the fingers and toes in children and anæmic girls. In the mild form there is a sensation of burning and itching, the part becomes swollen, of a dusky red colour, and the skin is tense and shiny. In more severe cases the burning and itching are attended with pain, and the skin becomes of a violet or wine-red colour. There is a third degree, closely approaching frost-bite, in which the skin tends to blister and give way, leaving an indolent raw surface popularly known as a “broken chilblain.”
Fig. 94.—Ulcerated Chilblains on Fingers of a Child.
Those liable to chilblains should take open-air exercise, nourishing food, cod-liver oil, and tonics. Woollen stockings and gloves should be worn in cold weather, and sudden changes of temperature avoided. The symptoms may be relieved by ichthyol ointment, glycerin and belladonna, or a mixture of Venice turpentine, castor oil, and collodion applied on lint which is wrapped round the toe. Another favourite application is one of equal parts of tincture of capsicum and compound liniment of camphor, painted over the area night and morning. Balsam of Peru or resin ointment spread on gauze should be applied to broken chilblains. The most effective treatment is Bier's bandage applied for about six hours twice daily; it can be worn while the patient is following his occupation; in chronic cases this may be supplemented with hot-air baths.
Boils and Carbuncles.—These result from infection with the staphylococcus aureus, which enters the orifices of the ducts of the skin under the influence of friction and pressure, as was demonstrated by the well-known experiment of Garrè, who produced a crop of pustules and boils on his own forearm by rubbing in a culture of the staphylococcus aureus.
A boil results when the infection is located in a hair follicle or sebaceous gland. A hard, painful, conical swelling develops, to which, so long as the skin retains its normal appearance, the term “blind boil” is applied. Usually, however, the skin becomes red, and after a time breaks, giving exit to a drop or two of thick pus. After an interval of from six to ten days a soft white slough is discharged; this is known as the “core,” and consists of the necrosed hair follicle or sebaceous gland. After the separation of the core the boil heals rapidly, leaving a small depressed scar.
Boils are most frequently met with on the back of the neck and the buttocks, and on other parts where the skin is coarse and thick and is exposed to friction and pressure. The occurrence of a number or a succession of boils is due to spread of the infection, the cocci from the original boil obtaining access to adjacent hair follicles. The spread of boils may be unwittingly promoted by the use of a domestic poultice or the wearing of infected underclothing.
While boils are frequently met with in debilitated persons, and particularly in those suffering from diabetes or Bright's disease, they also occur in those who enjoy vigorous health. They seldom prove dangerous to life except in diabetic subjects, but when they occur on the face there is a risk of lymphatic and of general pyogenic infection. Boils may be differentiated from syphilitic lesions of the skin by their acute onset and progress, and by the absence of other evidence of syphilis; and from the malignant or anthrax pustule by the absence of the central black eschar and of the circumstances which attend upon anthrax infection.
Treatment.—The skin of the affected area should be painted with iodine, and a Klapp's suction bell applied thrice daily. If pus forms, the skin is frozen with ethyl-chloride and a small incision made, after which the application of the suction bell is persevered with. The further treatment consists in the use of diluted boracic or resin ointment. In multiple boils on the trunk and limbs, lysol or boracic baths are of service; the underclothing should be frequently changed, and that which is discarded must be disinfected. In patients with recurrence of boils about the neck, re-infection frequently takes place from the scalp, to which therefore treatment should be directed.
Any impaired condition of health should be corrected; when, there is sugar or albumen in the urine the conditions on which these depend must receive appropriate treatment. When there are successive crops of boils, recourse should be had to vaccines. In refractory cases benefit has followed the subcutaneous injection of lipoid solution containing tin.
Carbuncle may be looked upon as an aggregation of boils, and is characterised by a densely hard base and a brownish-red discoloration of the skin. It is usually about the size of a crown-piece, but it may continue to enlarge until it attains the size of a dinner-plate. The patient is ill and feverish, and the pain may be so severe as to prevent sleep. As time goes on several points of suppuration appear, and when these burst there are formed a number of openings in the skin, giving it a cribriform appearance; these openings exude pus. The different openings ultimately fuse and the large adherent greyish-white slough is exposed. The separation of the slough is a tedious process, and the patient may become exhausted by pain, discharge, and toxin absorption. When the slough is finally thrown off, a deep gap is left, which takes a long time to heal. A large carbuncle is a grave disease, especially in a weakly person suffering from diabetes or chronic alcoholism; we have on several occasions seen diabetic coma supervene and the patient die without recovering consciousness. In the majority of cases the patient is laid aside for several months. It is most common in male adults over forty years of age, and is usually situated on the back between the shoulders. When it occurs on the face or anterior part of the neck it is especially dangerous, because of the greater risk of dissemination of the infection.
A carbuncle is to be differentiated from an ulcerated gumma and from anthrax pustule.
Fig. 95.—Carbuncle of seventeen days' duration in a woman æt. 57.
Treatment.—Pain is relieved by full doses of opium or codein, and these drugs are specially indicated when sugar is present in the urine. Vaccines may be given a trial. The diet should be liberal and easily digested, and strychnin and other stimulants may be of service. Locally the treatment is carried out on the same lines as for boils.
In some cases it is advisable to excise the carbuncle or to make incisions across it in different directions, so that the resulting wound presents a stellate appearance.
Acute Abscesses of the Skin and Subcutaneous Tissue in Young Children.—In young infants, abscesses are not infrequently met with scattered over the trunk and limbs, and are probably the result of infection of the sebaceous glands from dirty underclothing. The abscesses should be opened, and the further spread of infection prevented by cleansing of the skin and by the use of clean under-linen. Similar abscesses are met with on the scalp in association with eczema, impetigo, and pediculosis.
Veldt Sore.—This sore usually originates in an abrasion of the epidermis, such as a sun blister, the bite of an insect, or a scratch. A pustule forms and bursts, and a brownish-yellow scab forms over it. When this is removed, an ulcer is left which has little tendency to heal. These sores are most common about the hands, arms, neck, and feet, and are most apt to occur in those who have had no opportunities of washing, and who have lived for a long time on tinned foods.
Tuberculosis of the Skin.—Interest attaches chiefly to the primary forms of tuberculosis of the skin in



Comments (0)